Dr. Elias Darido is a fellowship-trained bariatric and weight loss surgeon who has performed over 1,000 gastric sleeve procedures at Houston Weight Loss Surgery Center. He is board-certified by the American Board of Surgery. He is a Fellow of the American College of Surgeons, and American Society of Bariatric and Metabolic Surgery with specialized training in minimally invasive and robotic weight loss surgery.
What Is Gastric Sleeve Surgery?
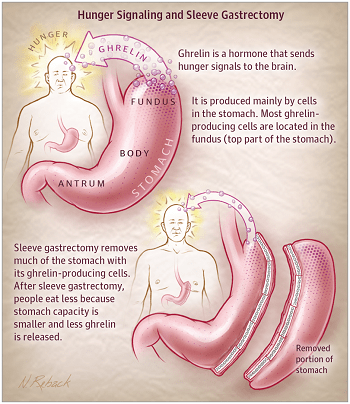
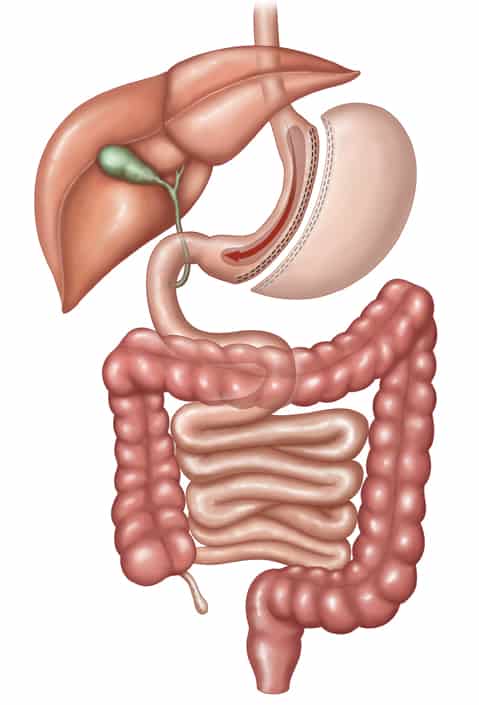
Gastric sleeve surgery, formally known as sleeve gastrectomy, is a weight loss procedure that permanently reduces the size of the stomach by approximately 75-80%. The surgeon removes the stretchable, curved portion of the stomach and shapes the remaining portion into a narrow tube or “sleeve” roughly the size and shape of a banana.
This smaller stomach physically limits how much food you can eat in one sitting. But the procedure does far more than just restrict portion size. By removing the portion of the stomach that produces ghrelin (the “hunger hormone”), gastric sleeve surgery fundamentally changes your appetite and hormonal signaling, making it easier to eat less without constantly fighting hunger.
Gastric sleeve surgery is currently the most commonly performed bariatric procedure in the United States. It accounts for more than 60% of all weight loss surgeries performed in Houston, TX. Its popularity is driven by its effectiveness, relatively straightforward technique, and lower complication rate compared to other bariatric procedures.
At a glance:
- Procedure time: 45-60 minutes
- Hospital stay: Typically 1 night (most patients go home same day)
- Time off work: 1 week for desk jobs, 4-6 weeks for physical labor
- Expected weight loss: 60-70% of excess body weight within the first 12-18 months
- Long-term success: Studies show sustained weight loss and improvement in obesity-related conditions at 5 and 10+ years
How Does Gastric Sleeve Surgery Work?
Gastric sleeve surgery works through two complementary mechanisms: restriction and hormonal change.
The Restrictive Component
During the procedure, roughly 75-80% of the stomach is permanently removed. The remaining stomach holds approximately 2-4 ounces of food immediately after surgery (compared to about 40 ounces for a normal stomach). Over time, the sleeve can stretch slightly to hold 4-8 ounces, but it will never return to its original size because the removed portion of the stomach is gone permanently.
This means you feel full after eating far less food, which naturally reduces your daily calorie intake.
The Hormonal Component
This is the most important part of weight loss that most patients don’t realize. Removing part of the stomach alters several hormones that control satiety, appetite, and insulin resistance. Ghrelin, the hormone that triggers hunger, decreases. Other hormones that control satiety, like GLP-1 (better known as Ozempic®, Wegovy®, and Mounjaro® commercially) increase after gastric sleeve surgery. As a result, patients report a significant decrease in appetite, fewer food cravings, and less preoccupation with eating. These changes begin almost immediately after surgery and persist long-term.
The procedure also improves insulin sensitivity and alters the production of other gut hormones involved in blood sugar regulation, which is why many patients with Type 2 diabetes see rapid improvement or complete remission even before significant weight loss occurs.
What Happens During the Procedure: Step by Step
- Anesthesia. You are placed under general anesthesia. The procedure is performed laparoscopically (minimally invasive) through 4-5 small incisions in the upper abdomen.
- The liver is gently retracted. The liver sits directly over the stomach. A small instrument holds it out of the way to expose the surgical area. This is why a pre-operative liver shrinking diet is required. It makes the surgery safer and technically easier.
- The stomach is freed from surrounding tissue. The surgeon carefully separates the stomach from the surrounding fat and blood vessels along the greater curvature (the outer, curved edge).
- The hiatal hernia is repaired. Most overweight patients have a hiatal hernia: the upper part of the stomach slides up into the chest through an opening in the breathing muscle. Hiatal hernias are associated with acid reflux, and if not repaired during gastric sleeve surgery, patients may continue to have or develop acid reflux and heartburn.
- A sizing tube (bougie) is placed. A calibrated tube is inserted through the mouth and into the stomach. This tube serves as a guide to ensure the remaining sleeve has a consistent and appropriate size. Dr. Darido uses a 40 French bougie, which is not too tight for complications, and not too loose for inadequate restriction. Dr Darido pays particular attention to preserving the natural angulation of the stomach at an area called the incisura angularis. This is where the horizontal and vertical parts of the stomach join. Narrowing this area by stapling too close to the bougie is a grave mistake that results in either staple line leak or severe acid reflux after surgery.
- The stomach is divided. Using a surgical stapler, the surgeon fires sequential staple loads along the length of the stomach, following the bougie. Each staple line both cuts and seals the stomach simultaneously. The staple line is typically reinforced with buttressing material to reduce the risk of leaks and bleeding. Dr. Darido does not over-sew the staple line so as not to distort the staples and cause unnecessary twisting in the sleeve contour.
- The removed stomach is extracted. The excised portion (roughly 75-80% of the original stomach) is removed through one of the small incisions.
- A leak test is performed. Before closing, the surgeon tests the staple line to ensure there are no leaks. For that purpose, an upper endoscopy is performed and air is injected into the submerged sleeve to check for any bubbles escaping from inside the stomach. (Air leak test)
- Incisions are closed. The small incisions are closed with absorbable sutures and covered with surgical glue or small bandages.
Gastric Sleeve Requirements: Am I a Candidate?
Standard Medical Criteria
Insurance companies and medical guidelines generally require the following:
- BMI of 40 or higher (approximately 75-100+ pounds overweight), OR
- BMI of 35-39.9 with at least one obesity-related health condition such as Type 2 diabetes, high blood pressure, sleep apnea, heart disease, fatty liver disease, or severe joint disease
- BMI of 30-34.9 with poorly controlled Type 2 diabetes (newer guidelines are expanding access to this group)
- Documented history of failed weight loss attempts through diet, exercise, and/or medication
- Medical clearance from your primary care physician and, in some cases, a cardiologist or pulmonologist
What Dr. Darido Evaluates Beyond BMI
Meeting BMI criteria doesn’t automatically mean surgery is the right next step. At Houston Weight Loss Surgery Center, every patient undergoes a comprehensive evaluation that includes:
- Nutritional assessment. Meeting with our registered dietitian to evaluate current eating habits, nutritional deficiencies, and readiness for the dietary changes required after surgery.
- Psychological evaluation. A meeting with a psychologist or licensed counselor who specializes in bariatric patients. This isn’t a barrier to surgery. It’s designed to ensure you have the support systems and coping strategies in place for long-term success.
- Medical workup. Lab work, EKG, and any specialty consultations needed based on your health history. Patients with sleep apnea will need a sleep study; patients with a history of acid reflux may need an upper endoscopy.
- Upper endoscopy (EGD). Dr. Darido performs a pre-operative endoscopy on all gastric sleeve candidates to evaluate for hiatal hernias, Barrett’s esophagus, and H. pylori infection. This is particularly important for Dr. Darido because untreated hiatal hernias can worsen acid reflux after sleeve surgery, and Barrett’s esophagus may require a different surgical approach.
Gastric Sleeve vs. Gastric Bypass: Which Is Right for You?
This is one of the most common questions patients ask. Both are excellent procedures, but they work differently and are suited for different patients.
| Gastric Sleeve | Gastric Bypass (Roux-en-Y) | |
|---|---|---|
| How it works | Removes ~80% of the stomach; no intestinal rerouting | Creates a small stomach pouch AND reroutes the small intestine |
| Procedure time | 45-60 minutes | 90-120 minutes |
| Expected excess weight loss | 60-70% in 12-18 months | 70-80% in 12-18 months |
| Malabsorption | No, nutrients are absorbed normally | Yes, reduced absorption of certain minerals and vitamins |
| Vitamin/supplement requirements | Daily multivitamin + B12 | More extensive supplementation required lifelong |
| Acid reflux impact | Eliminates reflux when properly done in addition to a concomitant hiatal hernia repair | Typically improves or eliminates reflux |
| Reversibility | Not reversible (stomach is removed) | Technically reversible but rarely done |
| Best for | Most bariatric candidates; simpler anatomy, lower complication profile | Patients with higher BMIs, or Type 2 diabetes requiring maximum metabolic effect |
| Revision options | Can be converted to bypass or duodenal switch if needed | Limited revision options |
Dr. Darido’s perspective: GLP-1 medications were developed based on bariatric and metabolic surgery mechanisms of action. You secrete GLP-1 after each meal. Gastric sleeve surgery enhances your own body’s GLP-1 secretion as well as other hormones to promote weight loss. Hence, GLP-1 injectables are a valuable weight loss medication and have helped many patients. However, they are less effective than bariatric surgery, especially in patients with morbid obesity. The weight loss is more modest, the medications must be taken indefinitely, and the long-term data beyond 3-5 years is still limited. For patients with BMI 35+, surgery offers a more durable, cost-effective solution with decades of outcome data supporting it. That said, some patients benefit from GLP-1 medications as a complement to surgery, for example to optimize weight loss before surgery or to address weight regain years after surgery.
Recovery After Gastric Sleeve Surgery
Week 1: Clear Liquids
- Clear broth, sugar-free Jell-O, water, diluted protein water
- Sip slowly. Your new stomach is healing and can only handle small amounts at a time.
- Walk frequently (hospital halls, then around the house) to promote healing and prevent blood clots
- Most patients manage pain with liquid Tylenol within 2-3 days
Weeks 2-3: Full Liquids
- Protein shakes, strained cream soups, Greek yogurt, milk
- Goal: 60-80g of protein per day (primarily from shakes at this stage)
- 64+ ounces of fluid daily (sipping throughout the day)
- Most desk-job patients return to work during this phase
Weeks 4-5: Soft/Pureed Foods
- Scrambled eggs, cottage cheese, soft fish, mashed beans, hummus, applesauce
- Introduce one new food at a time to identify anything that doesn’t sit well
- Begin establishing the eating habits that will carry you forward: eat slowly, chew thoroughly, stop when you feel full
Week 6+: Regular Diet (Modified)
- Gradual introduction of solid foods
- Continue prioritizing protein first at every meal, then vegetables, then complex carbohydrates
- Avoid carbonated beverages, high-sugar foods, and drinking with meals (wait 30 minutes before and after eating)
- Resume exercise: walking, swimming, light weights. Avoid heavy lifting until cleared.
What to Expect Long-Term
- Hair loss: Temporary hair thinning occurs in roughly 30-40% of patients between months 3-9. This is caused by the rapid weight loss and caloric reduction, not by the surgery itself. It resolves on its own as nutrition stabilizes.
- Excess skin: Patients who lose significant amounts of weight may have loose skin, particularly in the abdomen, arms, and thighs. Body contouring surgery is an option once weight has stabilized (typically 12-18 months post-op).
- Vitamins and supplements: Lifelong daily multivitamin, B12, calcium, and vitamin D are recommended. Your lab work will be monitored regularly to detect and correct any deficiencies.
- Follow-up schedule: Appointments at 2 weeks, 6 weeks, 3 months, 6 months, 1 year, and annually thereafter.
Gastric Sleeve Surgery Cost and Insurance
With Insurance
Gastric sleeve surgery is covered by most major insurance plans when medical necessity criteria are met. Typical requirements include documented BMI of 40+ (or 35+ with comorbidities), a history of supervised weight loss attempts, and completion of any insurance-mandated pre-surgical programs (often 3 months of documented physician-supervised weight management).
At Houston Weight Loss Surgery Center, our insurance coordination team handles prior authorization and benefits verification. We work with most major insurance carriers including Blue Cross, Aetna, Cigna, UnitedHealthcare. Out-of-pocket costs with insurance typically range from $0 to $5,000 depending on your plan’s deductible and coinsurance.
Without Insurance (Self-Pay)
For patients who are uninsured or whose insurance does not cover bariatric surgery, Houston Weight Loss Surgery Center offers self-pay pricing that includes the surgeon’s fee, anesthesia, hospital stay, and all routine follow-up care for less than $500 per month.
Self-pay pricing: $10,000 (all-inclusive)
We offer financing options through Cherry with monthly payment plans available. Contact our office for a personalized quote.
Is Gastric Sleeve Worth the Cost?
Consider the long-term comparison: a patient spending $300/month on GLP-1 medications will spend $36,000 over 10 years (with weight regain if they stop). A gastric sleeve is a one-time investment that delivers permanent anatomic change. Most patients also see significant reductions in medication costs for diabetes, blood pressure, cholesterol, and sleep apnea, savings that accumulate year after year.
Expected Weight Loss After Gastric Sleeve
- 3 months: 30-40% of excess weight lost
- 6 months: 50-60% of excess weight lost
- 12 months: 60-70% of excess weight lost
- 18 months: Maximum weight loss achieved for most patients (65-75% of excess weight)
- 5+ years: Most patients maintain 50-60% excess weight loss long-term
What does this look like in real numbers? A patient who is 5’6″ and weighs 280 pounds has approximately 130 pounds of excess weight (above an ideal weight of ~150). A 65% excess weight loss would mean losing approximately 85 pounds, bringing them to ~195 pounds.
Individual results vary based on adherence to dietary guidelines, exercise habits, metabolic factors, and follow-up compliance. Patients who attend regular follow-ups and engage with the nutritional support program consistently achieve better long-term outcomes.
Risks and Complications
Gastric sleeve surgery is considered safe, particularly when performed by an experienced bariatric surgeon at an accredited center. However, like any surgical procedure, it carries risks.
Serious but Rare Complications (<1%)
- Staple line leak: The most serious potential complication. A small opening along the staple line allows stomach contents to leak into the abdomen. Risk is approximately 0.5-1% with experienced surgeons using proper technique and staple line reinforcement.
- Bleeding: Post-operative bleeding from the staple line or surgical sites. Usually self-limited but may occasionally require intervention.
- Blood clots (DVT/PE): Risk is minimized through early mobilization, compression devices, and blood-thinning medication.
- Stricture: Narrowing of the sleeve that can cause difficulty swallowing or persistent vomiting. Usually treatable with an endoscopic balloon dilation.
Common and Expected Side Effects
- Nausea: Common in the first few weeks, especially if eating or drinking too quickly
- Acid reflux: New or worsened GERD only if the gastric surgery is not properly performed.
- Food intolerances: Certain foods may not sit well after surgery, particularly red meat, bread, pasta, and fibrous vegetables. These often improve over time.
- Dumping syndrome: Less common with sleeve than bypass, but can occur. Characterized by nausea, cramping, and diarrhea after eating high-sugar foods.
Dr. Darido’s Complication Rates
Dr. Darido has performed over 1,000 gastric sleeve procedures with a leak rate of 0% and an overall complication rate of less than 1%, which is below the national average.
Before and After: Patient Results
 For additional insight into patient experiences, readers are encouraged to visit our Patient Reviews page, where individuals share their journeys, outcomes, and what life has been like after bariatric surgery.
For additional insight into patient experiences, readers are encouraged to visit our Patient Reviews page, where individuals share their journeys, outcomes, and what life has been like after bariatric surgery.
Frequently Asked Questions
How long does gastric sleeve surgery take?
The procedure typically takes 45-60 minutes. Including pre-operative preparation and post-operative recovery room time, plan for approximately 3-4 hours total at the hospital.
How much weight will I lose with a gastric sleeve?
Most patients lose 60-70% of their excess body weight within 12-18 months. For someone 100 pounds overweight, that translates to approximately 60-70 pounds of weight loss.
Is gastric sleeve surgery reversible?
No. Unlike gastric bypass (which is technically reversible) or the gastric band (which is removable), the gastric sleeve is permanent because the removed portion of the stomach is physically taken out of the body. However, the sleeve can be revised or converted to a gastric bypass or duodenal switch if needed in the future.
How long do you stay in the hospital after gastric sleeve?
Most patients are candidates for same-day discharge depending on their medical history and how they’re recovering. Some patients stay 1 night in the hospital.
Can you drink alcohol after gastric sleeve?
Alcohol is not recommended for at least 6 months after surgery. After that, alcohol should be consumed very cautiously. Your smaller stomach absorbs alcohol faster, meaning you’ll feel the effects more quickly and intensely. Alcohol is also high in empty calories and can contribute to weight regain.
Will I need plastic surgery after losing weight?
Not everyone does. It depends on how much weight you lose, your age, skin elasticity, and genetics. Patients who lose 80+ pounds are more likely to have excess skin. Body contouring options include abdominoplasty (tummy tuck), brachioplasty (arm lift), and thigh lift. These are typically considered 12-18 months after surgery once weight has stabilized.
What if I have acid reflux — can I still get a gastric sleeve?
Yes, you can get a gastric sleeve if you have GERD and acid reflux. A properly performed gastric sleeve surgery and a concomitant hiatal hernia repair alleviate all GERD related symptoms.
How does gastric sleeve compare to Ozempic or Wegovy?
Gastric sleeve surgery produces significantly more weight loss (60-70% of excess weight vs. 15-22% of total body weight with GLP-1s), the results are permanent without ongoing medication, and it has higher rates of diabetes remission. GLP-1 medications require lifelong use to maintain results and cost $800-1,500/month. Surgery is a one-time procedure. Both are valid tools, and some patients benefit from a combination approach.
What is the gastric sleeve failure rate?
Approximately 10-20% of patients may not achieve their expected weight loss goals or may experience significant weight regain over time. The most common causes of suboptimal results are return to pre-surgical eating habits, inadequate follow-up, and untreated emotional eating. Patients who remain engaged with their surgical team, attend follow-ups, and maintain lifestyle changes have the best long-term outcomes. Revision surgery or conversion to gastric bypass is an option for patients who experience weight regain.
Is gastric sleeve surgery the right choice for me?
For most people considering weight loss surgery, the answer is yes. Gastric sleeve is the most commonly performed bariatric procedure in the United States. It is less invasive than gastric bypass and significantly more effective than lap band surgery. When performed correctly, it has a low complication rate and produces lasting weight loss results.
The key to a successful sleeve is complete removal of the upper portion of the stomach, called the gastric fundus. This step reduces hunger hormones, helps you feel full sooner, and lowers the risk of acid reflux after surgery. Schedule a consultation so we can review your health history and goals to confirm whether sleeve surgery is the right fit for you.
Does the size of the surgical tool affect how much weight I lose?
Not significantly. Surgeons have debated the size of the tube used to shape the sleeve for years, but research shows that what matters most is how thoroughly the upper portion of the stomach is removed. Patients who have leftover stomach tissue in that area tend to feel less full, lose less weight, and experience more acid reflux after surgery, regardless of what size tool was used.
Dr. Darido focuses on complete removal of this portion and pays careful attention to the natural curve of the stomach during the procedure. This precision reduces complications and gives you the best possible long-term result.
What happens if too much stomach is left behind during sleeve surgery?
If the upper portion of the stomach is not fully removed, the hunger hormone it produces stays active. That means ongoing hunger, less predictable weight loss, and a higher chance of acid reflux. Patients in this situation sometimes need a revision procedure to complete the removal.
Research shows that patients who underwent revision surgery to correct an incomplete sleeve lost an additional significant amount of excess weight on average, and many saw their reflux symptoms improve. This is one of the reasons surgical technique at the time of your original procedure makes such a difference in long-term outcomes.
Why Choose Houston Weight Loss Surgery Center

Specialized bariatric focus. Dr. Darido is a fellowship-trained bariatric surgeon, not a general surgeon who occasionally performs weight loss procedures. This specialization means refined technique, lower complication rates, and a team that understands the unique needs of bariatric patients.
Comprehensive program. Surgery is only one part of the equation. Houston Weight Loss Surgery Center provides a full continuum of care including nutritional counseling, psychological support, support groups, and long-term follow-up. Our program is designed for patients who want lasting results, not just a quick fix.
Full-spectrum expertise. Dr. Darido performs all major bariatric procedures (gastric sleeve, gastric bypass, and revision surgery) as well as foregut surgery for acid reflux and hiatal hernias. This means your likelihood of getting acid reflux after gastric sleeve surgery is very close to zero. Our procedure recommendation is based on what’s best for YOU, not on what the surgeon is most comfortable performing.
Serving Houston and surrounding communities. Patients travel from across Greater Houston, including The Woodlands, Katy, Sugar Land, Pearland, Pasadena, League City, and Galveston for their bariatric care at Houston Weight Loss Surgery Center.
Related Procedures
- Gastric Bypass Surgery — The traditional bariatric procedure
- Sleeve Revision Surgery — Options if your sleeve isn’t delivering results
- Lap Band Removal & Conversion — Converting from a band to a sleeve
- Endoscopic Sleeve Gastroplasty (ESG) and gastric balloon — Non-surgical alternatives that we do not recommend because of poor weight loss outcome
Take the Next Step
Schedule a consultation with Dr. Darido to find out if gastric sleeve surgery is right for you. During your visit, we’ll review your medical history, discuss your weight loss goals, and outline a personalized plan, whether that’s surgery, medication, or a combination approach.
About the Author
Dr. Darido, MD, FACS
Dr. Elias Darido is a board-certified bariatric and foregut surgeon and the founder of Houston Weight Loss Surgery Center. He completed his bariatric surgery fellowship at the University of North Carolina in Chapel Hill, and has performed over 1,000 weight loss procedures. He is a member of the American Society for Metabolic and Bariatric Surgery (ASMBS), a Fellow of the American College of Surgeons, and a recognized expert in gastric sleeve surgery, revision bariatrics, and the management of acid reflux after weight loss surgery.