Endoscopic procedures for treatment of obesity and GERD are flooding the market these days. The FDA has approved a number of devices like TIF and MUSE for GERD treatment and the Intragatric Balloon for weight loss. These devices are introduced as a “bridge” between medical therapy and surgery. They are praised as much needed tools to fill in the “gap” in the treatment of two disease that have reached an epidemic level in our society. Access to surgery is limited for various reasons. Cost and fear of surgery are common barriers between patients and surgical procedures. Along those lines, the newly acclaimed endoscopic sleeve gastroplasty for treatment of obesity is introduced.
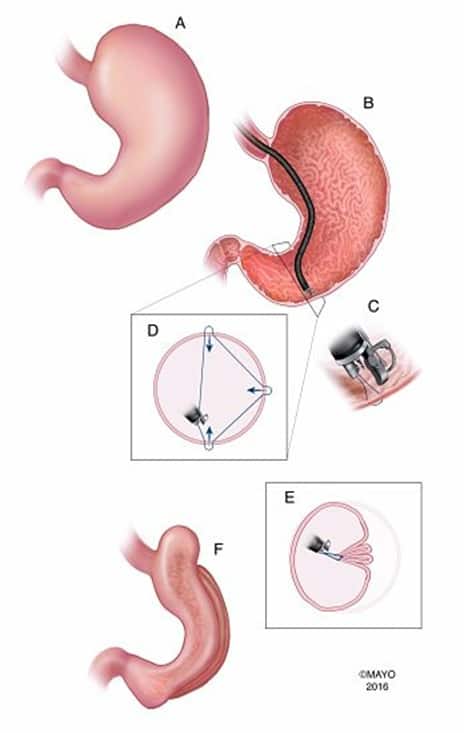
Endoscopic sleeve gastroplasty is an outpatient procedure performed through the mouth using endoscopic suturing. It is less invasive than a sleeve gastrectomy and costs much less than traditional laparoscopic surgery. The stomach volume is reduced forcing the patient to eat less. The authors, however, who developed this procedure, claim that it reduces gastric emptying and attributes this fact to promoting satiety and delaying hunger. In their study published in Clinical Gastroenterology and Hepatology, 25 obese patients underwent this procedure with 3 suffering from serious complications including a pulmonary embolus and leak. This is equivalent to 4% leak rate. A very high number when compared to current gastric sleeve or bypass surgery series. Four of the participants were tested for gastric emptying and showed slowing of gastric emptying of solids.
No doubt that this procedure contradicts everything we know about sleeve gastrectomy mechanism of action. Gastric sleeve surgery entails the complete resection of the gastric fundus leading to accelerated gastro-duodenal food emptying. Rapid food delivery to the distal intestine stimulates the secretion of certain gut hormones like GLP-1 that promote satiety, decrease hunger and postprandial blood sugar. Endoscopic sleeve gastroplasty leaves a big part of the gastric fundus un-resected and delays gastric emptying.
Is it possible for two opposing mechanism to lead to weight loss? I seriously doubt it. We invite our gastroenterology colleagues at the Mayo Clinic in Rochester to reconsider their position on means of altering gastric physiology to achieve weight loss. Reorienting their research towards promoting gastric emptying using innovative technology may help millions of obese and diabetic patients worldwide.