The incisura angularis is the Achilles heel of sleeve gastrectomy. Preserving this natural gastric angulation is crucial to ensure proper weight loss while preserving basic gastric anatomy and function. Stapling too close to the incisura angularis results in sharp angulation in that area that causes functional obstruction. Functional obstruction of the gastric sleeve lumen increases the risk of postoperative staple line leak, decreases weight loss and precipitates acid reflux.
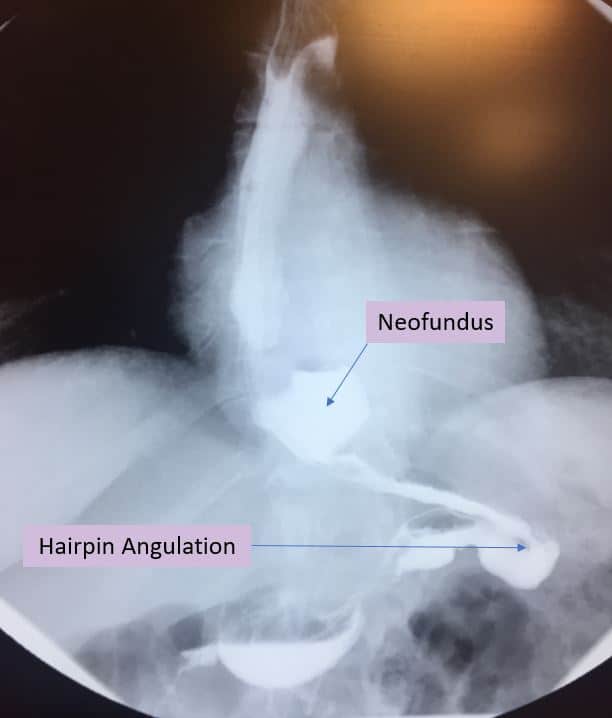
Chronic functional obstruction of gastric sleeve lumen results in increased intra-gastric pressure and proximal lumen dilation. The upper part of the sleeve enlarges with time leading to the creation of a neo-fundus. The upper part of the sleeve is more prone to dilation due to its thin and compliant wall. Furthermore, a small dog ear is typically left to decrease leak rate. This small residual gastric fundus has a larger diameter than the rest of the gastric sleeve lumen. The larger the lumen diameter, the higher is wall tension leading to more stretching and dilation. Indeed, the presence of a neo-fundus as the attached UGI picture depicts is an indirect sign of functional obstruction. Chronic obstruction also results in anterior and medial rotation of the gastric sleeve proximal to the incisura angularis resulting in the classic hairpin deformity and further accentuating the sharp angulation and obstruction.
Patients typically present with worsening acid reflux related symptoms poorly controlled with proton pump inhibitors. The combination of poor gastric motility, high gastric pressure and gastric fluid secretion accumulation in the neo-fundus results in severe reflux into the esophagus. The only effective solution in this case is to convert the gastric sleeve into a Roux-en-Y gastric bypass. The conversion is straightforward, effective and safe. Gastric bypass restores normal gastrointestinal motility. It immediately relieves all GERD related symptoms and promotes weight loss.
In summary, avoiding narrowing at the incisura angularis cannot be over-emphasized. Sleeve gastrectomy is a mutilating procedure but preserving basic gastric anatomy and function is mandatory to avoid complications. Gastric fundus invagination, a weight loss procedure that I have developed few years ago has the advantage of preserving gastric structure while modifying gastric emptying, and food interaction. Gastric fundus invagination or sleeve gastrotomy as Dr. Mason would like to call it has the potential of becoming the first line treatment for morbid obesity.