
Several studies have shown that a two-stage conversion of lap band to gastric sleeve is safer than a single stage approach. In the current issue of Surgery for Obesity and Related Diseases, a group of bariatric surgeons from Saudi Arabia demonstrate that a single stage approach is safe and effective. The study is based on a single-surgeon prospective database and included 209 band to sleeve conversions. Only one patient of the 209 conversions developed a staple line leak.
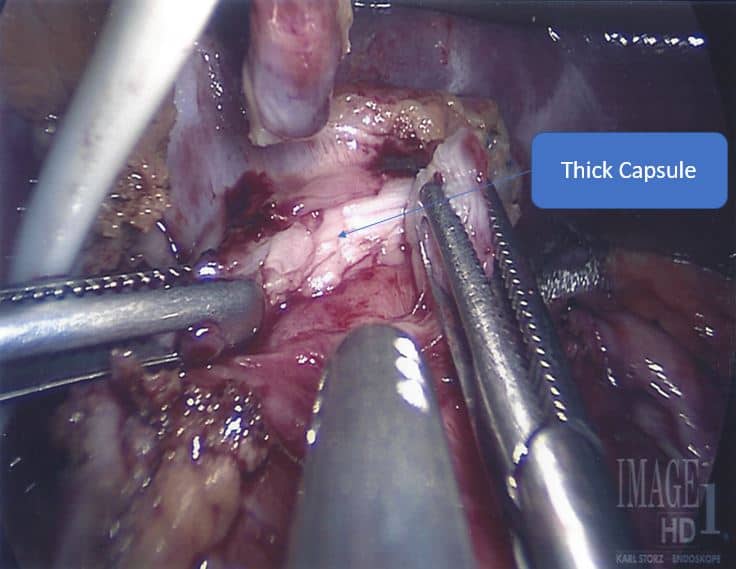
The lead author reports that key to avoiding complications in one stage band to sleeve revisions is meticulous and complete dissection of the fibrous capsule surrounding the stomach at the band site. The capsulotomy is started at the level of the left crus muscle and extended anteriorly to release any tethered gastric wall and fully mobilize the gastric pouch above the band. The author further recommends that the gastric pouch that is often dilated must be completely resected to avoid leaving behind a high-pressure area that may lead to increased leak rate.
This photo illustrates the technique described whereby the fibrous capsule is dissected prior to stapling.
At Houston Weight Loss Surgery Center, we advocate a two-stage band to sleeve revision. Most published studies have shown increased leak rate following revision bariatric surgery in general and the one stage band to sleeve conversion. This is due to several theoretical factors like scar tissue formation, decreased blood supply, dilated and inflamed gastric tissue above the band as well as increased gastric pouch pressure and esophageal dysmotility. Pseudo-achalasia secondary to gastric banding is not uncommon. Revising a lap band to a high-pressure system like gastric sleeve may increase the intra-luminal pressure at the gastro-esophageal junction especially in pseudo-achalasia cases. This may potentially contribute to increased staple line leak rate. Interestingly, one stage lap band to gastric bypass revision is not associated with increased leak rate. This may be due to the negative pressure system created by the Roux-en-Y configuration. At Houston Weight Loss Surgery center, we routinely offer a one stage band to gastric bypass revision.
To summarize, scar tissue dissection and removal is a must. However, removing the fibrous capsule by itself is unlikely to decrease the sleeve leak rate as other factors are at play. I do agree with the author that the capsule must be removed completely to release the gastric wall and prevent stapling part of the capsule. We have adopted this approach several times and had no leak. However, I do not consider the one stage approach to be a standard of care. It is not superior to the two-stage revision. I prefer for the inflammation and fibrosis to heal and gastric tissue as well as esophageal function to recover over a 6-month period prior to gastric sleeve resection. If the patient insists on a one stage approach for insurance or financial reasons we offer lap band to gastric bypass revision as the safest and most effective solution.